Round 27
Round 27 GPC home Rounds Resources Contacts Survey instrumentsWill be shared soon…

Through a collaboration between the MRC and UVRI in 1989, the GPC was established in Kyamulibwa sub county, Kalungu district.
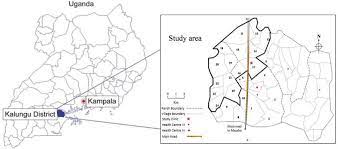
It comprises a population of around 22,000 people within 25 adjacent study villages. Its original aim was to study the epidemiology of HIV/ AIDS in the general population, and data from the GPC has made major contributions to our understanding of the changing patterns of HIV and informed policy and practice both in Uganda and internationally. Over time, research at the GPC has expanded to address scientific questions on other infectious diseases and non communicable diseases (NCDs), ranging from basic science, epidemiology, social science and intervention research.
The GPC is the source of rich longitudinal population and clinic data since. This data, as well as other demographic, epidemiological and genomic data from individual external projects, are extensively linked and shareable. This provides an important resource for future studies, and the Unit is actively increasing this data’s access.
Similarly, we have long-term blood samples for every survey round since 1989, as well as samples from other projects. The samples are available for answering research questions for both Unit and external scientists; more than 40 papers have been published in the quinquennium, based on analyses of historical serum samples. These stored samples also make the GPC particularly attractive for future field research because they provide the ability to compare data historically.
The GPC provides a solid platform for population-based research, which has been crucial in improving our understanding of HIV. More recently, this dynamic structure proved critical in studies on community transmission and impact of SARS-COV2 (COVID-19). Thus, the GPC is not only a source of rich longitudinal data to do your data, but also a resource to embed numerous short-term externally funded studies. It supports all our research themes.